Increased healthcare security risks due to Roe v Wade reversal

Image by senivpetro via Freepik
With the Supreme Court overturning of the 1973 Roe v. Wade case that legalized abortion nationwide, multiple downstream effects may impact healthcare security. Now that abortion legality is determined by each individual state, healthcare security faces a challenging environment as they try to understand how laws will be implemented and enforced (civil vs. criminal).
To prepare for the unexpected, healthcare facilities (HCFs) and security teams should take the following recommendations and the necessary steps to best protect the safety and security of patients and healthcare professionals.
The Numbers
First, let's look at statistics to set the stage. In 2019, CDC and Guttmacher’s reported that there were 629,898 and 930,160 “legal” abortions nationally that year, slightly up from 2018. CDC says that in 2019, there were 11.4 abortions in the U.S. per 1,000 women ages 15 to 44. As of 2019, CDC reported that 9.3% of the abortions were performed on women whose state of residency was known to be different than the state where the abortion occurred.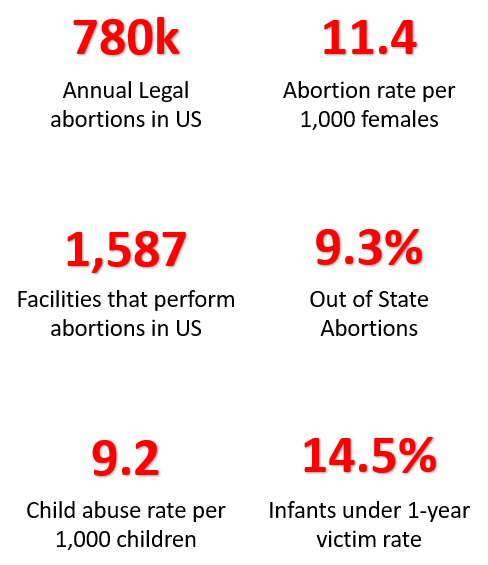 CREDIT: CDC
CREDIT: CDC
Figures reported are based on reports from clinics, hospitals, or physician offices and include the use of abortion pills at these sites. The number of sites that provide legal abortions has steadily decreased year over year since 1982, with an estimated total of approximately 1,587. There are currently eight states that have completely banned abortion; four states banned it after six weeks; and several other states banned it after 20+ weeks.
Several states are enacting the trigger law, which allows legal abortions for females that were raped or to save the life of the mother. According to RAINN, there are, on average, 463,000 victims of rape and sexual assault each year in the U.S. Approximately 250,000 of those raped are females of childbearing age. In addition, 94% of women raped experience some form of post-traumatic stress disorder (PTSD).
According to the Office of the Administration for Children & Families, in 2020, 9.2 per 1,000 children will be child victims of maltreatment or safety. Of those, 14.53% occur in infants under 12 months of age. Research shows that Shaken Baby Syndrome is the leading cause of child abuse deaths in the U.S. With over 1,300 cases per year, 80% of survivors suffer permanent damage, and 25% of SBS victims die.
Lastly, National Abortion Federation reported an increase in violence in 2021. Research shows a significant increase in stalking, blockades, hoax devices or suspicious packages, invasions, and assault and battery.
Impact on Healthcare Security
While it is difficult to predict all the impacts the overturn of Roe v Wade may have on HCF security, below are a few examples that are top of mind based on systems theory and downstream effects.
- Influx of infant and maternal population: The maternity and post-partum units may start to see an increase of infant births, both healthy and in need of critical neonatal care. If a hospital is currently working at bed and/or crib capacity, hospitals may need to overflow into other units.
- Safe Havens: We rarely talk about this, but there is a risk for an infant to be dropped off at or near the front door or lobby of HCFs. Safe Haven sites allow mothers of newborns to surrender unharmed babies to designated facilities within weeks of birth without fear of being prosecuted.
- Mental Health: Studies have found that females carrying an unwanted fetus experience higher rates of mental health issues. They tend to have higher rates of drug and alcohol use and higher rates of suicide or attempts for suicide.
- Child Protection Services (CPS): With the potential of increased birth rates, there may be an increase in CPS cases related to maltreatment or abuse. Engagements between CPS and families in HCFs may bring additional violence into the unit or facility.
- Shaken Baby Syndrome (SBS): With over 1,300 cases per year, 80% of survivors suffer permanent damage, and 25% of SBS victims die. CPS and law enforcement will be engaged in these cases. There are several security risks associated with these cases, such as safeguarding the infant, participating in law enforcement investigations, infant abduction, etc.
- Reporting of illegal abortions: Healthcare providers are required to report illegal activity to law enforcement. Clinicians forced to report illegal abortions could result in bullying, retaliation, or other workplace violent events. In addition, HCFs reporting of illegal activity could bring law enforcement investigations into the facility and require additional security resource support.
- External Threats: The rise in external verbal threats and physical violence targets HCFs, clinics, physician offices, and physicians that perform abortions. While most individuals are anti-abortion extremists, they also include local groups affiliated with churches or social gatherings.
HCF safety and security considerations include:
Risk Assessments:
- HCFs should conduct an environmental risk assessment to identify criteria that they would consider overflow infant and/or maternal patients into other areas within the facility.
- HCFs should ensure that maternal or infant employees and security personnel are well (educated and competent) in all infant security measures, including abuse, neglect and SBS.
- HCF should review the internet and social media posts to identify any risks that may bring violence from external threats. HCFs should collaborate with clinicians that may perform abortion procedures that are on HCF grounds and/or property or affiliated with the facility in any security measures.
- HCF security professionals should ensure that they have appropriate security equipment (access control, duress, cameras, patient protection, wayfinding signage) to accommodate patient influx and increased security risks.
Safe Havens:
- HCFs should validate that on-duty hospital staff receive information about Safe Haven laws and facility policy and procedures.
- Security patrolling and monitoring the environment to ensure a baby is not placed in an unsafe location, especially in extreme weather conditions.
Child Protection Services/Shaken Baby Syndrome:
- HCFs interdisciplinary teams (physicians, nurses, social services, bio-ethics members, risk and security) should convene to and develop procedural plans to mitigate risks. Plans should consider a specific location within the HCF to meet law enforcement and families.
- Security should coordinate with risk management and case managers/social workers in SBS cases to ensure the safety of the child and escort family, friends and government agents.
Workplace Violence (WPV):
- HCFs should consider implementing walk-through metal detectors at building entrances to prevent the opportunity of violence due to weapons or firearms.
- HCFs should review workplace violence and bullying training and reporting procedures. HCF should include human resources, risk management, and medical staff services in WPV teams.
- HCFs should collaborate with clinicians or physicians that have offices or clinics to ensure their employees receive appropriate WPV training and tools to mitigate them.
Looking for a reprint of this article?
From high-res PDFs to custom plaques, order your copy today!